Many untreated sprained ankles heal incorrectly, leaving the athlete with a stiff or weakened ankle, which is at a higher risk of re-injury.
Anatomy of the Ankle Joint
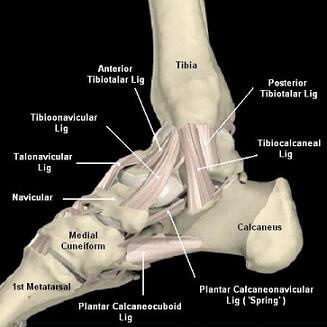
The ankle’s stability is provided by a number of ligaments, located on either side of the ankle joint, that are designed to protect the joint from excessive movement. On the inside of the ankle, the deltoid ligament, forms a dense strong supporting structure and consists of the tibionavicular, tibiocalcaneal and tibiotalar (anterior and posterior) ligaments. The lateral ligament complex (outside) consists of the weaker anterior talofibular, calcaneofibular and posterior talofibular ligaments.
What causes an ankle sprain?
An ankle sprain occurs when the ankle joint is taken beyond their normal range of movement and results in tearing of some of the above mentioned ligaments. Tearing is graded as:
- Grade 1: Mild: Involves a ligament stretch and no joint instability
- Grade 2: Moderate: Partial ligament tearing and some loss of joint stability
- Grade 3: Complete: Complete ligament rupture and abnormal joint motion and instability.
The most common mechanism of injury is when the foot lands awkwardly, resulting in the ankle joint suffering an inversion injury (i.e. the foot rolls inwards). This is often combined with a pointed foot, and results in the lateral structures becoming damaged. This is the most common type of ankle injury that occurs in sport, particularly those involving running, jumping and change of direction activities i.e. netball, basketball and all forms of football (soccer, rugby, Australian rules).
What are the symptoms?
- Pain and difficulty weight-bearing / walking
- Swelling, that may occur either quickly (less than 30 minutes) or later that day
- Restriction in ankle movement
- Giving way or a feeling of instability, particularly on un-even ground or when changing directions
- Recurrent clicking
What to do?
Rehabilitation is necessary to strengthen the ankle joint (and its associated structures) to withstand the strenuous demands required during activities of daily living and playing sport.
What can be done?
Physiotherapy management will involve a thorough physical and biomechanical assessment to assess the extent of your injury and proceed with any further investigations deemed necessary (i.e. x-ray if there is a concern of possible bone fracture). If the physiotherapist is satisfied that the injury only involves soft tissue structures, then treatment can commence immediately.
The rehabilitation program is based on an abundance of scientific research led by physiotherapists and is concentrated on immediate and correct management of the sprain during the acute inflammatory phase. This will assist in speeding up your recovery, while also allowing the repair phase of healing to proceed as soon as possible, to enable a successful recovery and return to sport. This program includes:
- RICE: this will prevent the ankle joint and its associated damaged structures becoming more sensitive and painful, and involves:
- Rest: by restricting loading on the ankle joint, it will minimise any further damage to your injured ankle. This may involve the use of crutches, braces and / or taping.
- Ice: regular application of ice will provide pain relief and minimize associated secondary soft tissue damage.
- Compression: minimise secondary damage and swelling to neighbouring soft tissues.
- Elevation: to assist in minimising ankle / foot swelling, by improving return blood flow to the heart.
- Massage: plays an important role with healing of the damaged ligaments by improving local blood flow and releasing adhesions between the collagen fibres that compose the ankle ligaments. This ensures they re-form appropriately, minimizing the development of any scar tissue in the ankle joint and / or ligamentous structures.
- Increase Strength: by a series of graduated exercises to the muscles of the lower leg, to improve the range of movement and the control of the ankle joint.
- Proprioceptive (Balance) Exercises: these will promote good foot positioning prior to landing and improve postural control. This is the most important part of the rehabilitation program, as it will significantly lower the risk of ankle re-injury.
- Stretching: poor gastrocnemius / soleus muscle flexibility can overload the ankle joint and associated foot structures. Hence, a regular stretching program to maximize their length is essential for correct ankle function.
- Correction of Pre-Disposing Factors: this ensures that the problem doesn’t re-occur and can include:
- Education on correct training principles of duration, intensity and frequency, to ensure the ankle can progressively adapt to the demands placed upon it with training.
- Biomechanical factors such as over-pronation (flattening) of the feet can cause excessive demands on the joints and muscles of the lower leg. Wearing appropriate running shoes for your foot type will minimise these problems. An assessment by our sports podiatrist maybe appropriate to determine whether orthotics are required to assist with this stability.
- Surgery: can be a possibility with long-standing ankle instability caused by recurrent ankle sprains. If conservative physiotherapy rehabilitation fails, an appropriate referral to a foot orthopaedic surgeon for further investigations (Bone scans, CT, MRI) can assist in ongoing management and to determine whether surgery is appropriate.

